Education
Penn State University (PSU): (State College/University Park, PA) [1962-1965]
UNDERGRADUATE COLLEGE [1962-1965]: Dr. Myers attended Penn State University, having graduated in 3 years with a B.S. (bachelor of science) degree (Cum Laude and Phi Beta Kappa). In that he had been such a poor grade school & high school student, it was a great and pleasant surprise to his parents. It was such a surprise that his father permanently labeled him "THE ENIGMA"!
Later in life, when colleagues questioned this circumstance, wondering how such a situation could occur, he explained that he had had an "INTRAVENOUS IQ INFUSION". This occurred when he finally realized that he had a VERY LOW MILITARY DRAFT NUMBER, and if he did not become a good student ASAP, he was headed to Vietnam in the infantry!
University of Pennsylvania School of Medicine (Renamed in 2011)
PERELMAN SCHOOL OF MEDICINE AT THE UNIVERSITY OF PENNSYLVANIA (Philadelphia Pennsylvania)
MEDICAL SCHOOL [1965-1969]. Founded in 1765, this is a private, Ivy League research university. It is the OLDEST MEDICAL SCHOOL IN THE UNITED STATES. It is ranked 3rd among medical schools in the United States, with a matriculation rate of 2.4% and a mean GPA of 3.94. (According to U.S. News & World Report). There are over 2900 faculty members, 1200 residents and fellows, and 775 M.D. students and nearly $1 billion in annual sponsored program awards.
During the summers he worked in the University of Pennsylvania veterinary neuroscience labs, with the hope of pursuing neurology as a specialty. During his medical school years, he met a fellow student, Dr. Jon Dranov, and they became med school pals and roommates and lifelong friends. Almost all med school vacation time was spent in Chester, Pennsylvania, with the Dranov family. After graduation, Dranov matched internships at Duke University Medical Center and Myers at the University of Pittsburgh Medical Center. Eventually, Dr. Dranov moved back to Penn State University, Myers' hometown, and started a large “world-class” multispecialty group consisting predominantly of American-trained med school professors.

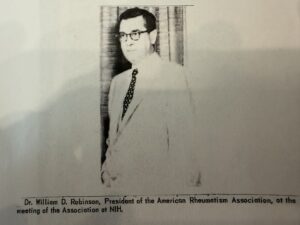
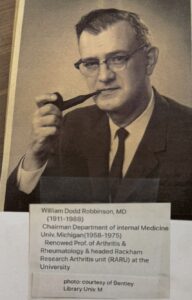 In the summer between the junior and senior years, Myers Penn. Med advisor suggested that if he wanted to become an expert on the physical exam, then he should consider spending a few months at the University of Michigan with William D. Robinson, MD. chairman of the Department of Internal Medicine, University of Michigan (1958-1975). Myers recalls being accepted as an extern to Dr Robinson. He recalls the challenge of finding temporary housing nearby since it was a time of the Ypsilanti murders and the Ypsilanti floods. The first day of Robinson rounds was most memorable: Myers, along with a group of interns residents and Rheumatology fellows evaluated a gentleman with Ankylosing Spondylitis (Marie Stumpel spondylitis). The patient was complaining of neck pain. Dr. Robinson turned to Myers and asked him, “where do you think this disease started”? Myers recalls thinking that this might be a trick question and wisely stated that he had not studied about this disease and was unsure.” “Fine, Robinson answered, I suggest when you get home this morning you look this up in Beeson and McDermotts Textbook of Medicine”.
In the summer between the junior and senior years, Myers Penn. Med advisor suggested that if he wanted to become an expert on the physical exam, then he should consider spending a few months at the University of Michigan with William D. Robinson, MD. chairman of the Department of Internal Medicine, University of Michigan (1958-1975). Myers recalls being accepted as an extern to Dr Robinson. He recalls the challenge of finding temporary housing nearby since it was a time of the Ypsilanti murders and the Ypsilanti floods. The first day of Robinson rounds was most memorable: Myers, along with a group of interns residents and Rheumatology fellows evaluated a gentleman with Ankylosing Spondylitis (Marie Stumpel spondylitis). The patient was complaining of neck pain. Dr. Robinson turned to Myers and asked him, “where do you think this disease started”? Myers recalls thinking that this might be a trick question and wisely stated that he had not studied about this disease and was unsure.” “Fine, Robinson answered, I suggest when you get home this morning you look this up in Beeson and McDermotts Textbook of Medicine”.
Myers said to himself, that was easy enough, just dodged a bullet. However, on arriving home and going to the recommended chapter, low and behold the author of the chapter DISEASES OF THE JOINTS ,was none other than Dr. Robinson!
Thereafter Myers tried to get the names of the patients for next-days rounds and study about them the night before.
 Seven days a week, rounds started at 6:30 AM. From this intense, three – month experience, he learned the art of comprehensive structured physical exams, which he applied to all patients the rest of his practicing life. Myers was most appreciative of this experience and each time he did a physical exam he was reminded of how this came to be. So, each Christmas thereafter for 10 years, he wrote a handwritten note thanking him, but there was never a response from Dr. Robinson. On the 11th year, he received a detailed letter, from Robinson ‘s hospital bed stating that he was indeed most appreciative for the 10 years of past letters, apologizing for not responding earlier!
Seven days a week, rounds started at 6:30 AM. From this intense, three – month experience, he learned the art of comprehensive structured physical exams, which he applied to all patients the rest of his practicing life. Myers was most appreciative of this experience and each time he did a physical exam he was reminded of how this came to be. So, each Christmas thereafter for 10 years, he wrote a handwritten note thanking him, but there was never a response from Dr. Robinson. On the 11th year, he received a detailed letter, from Robinson ‘s hospital bed stating that he was indeed most appreciative for the 10 years of past letters, apologizing for not responding earlier!
University of PittsburghInternship (Internal Medicine) [1969-1970]
Founded: 1886
 In 1969, Myers moved from Philadelphia to Pittsburgh, Pennsylvania, to start an internship. As a PITT medical intern, he was on call every other night, having a maximum supervised learning experience. At that time, Dr. Jack D. Myers was chairperson of the University of Pittsburgh Department of Medicine (1950–1970), no relationship to Myers. J. D. Myers, was not known for patience and was considered authoritarian. J.D. could accept "I do not know," but he could not accept excuses. He had 3 rules: punctuality, attention to detail, and a commitment to excellence. He had uncompromising standards and insisted we all live up to them. His strict code and no-nonsense training methods cultivated a cadre of dedicated physicians and revolutionized the University of Pittsburgh medical school. Physicians from all over the country contacted him about challenging cases that stumped them. He is said to have INFLUENCED THE WHOLE FIELD OF INTERNAL MEDICINE AND EVENTUALLY HELPED BRING IT INTO THE COMPUTER AGE.
In 1969, Myers moved from Philadelphia to Pittsburgh, Pennsylvania, to start an internship. As a PITT medical intern, he was on call every other night, having a maximum supervised learning experience. At that time, Dr. Jack D. Myers was chairperson of the University of Pittsburgh Department of Medicine (1950–1970), no relationship to Myers. J. D. Myers, was not known for patience and was considered authoritarian. J.D. could accept "I do not know," but he could not accept excuses. He had 3 rules: punctuality, attention to detail, and a commitment to excellence. He had uncompromising standards and insisted we all live up to them. His strict code and no-nonsense training methods cultivated a cadre of dedicated physicians and revolutionized the University of Pittsburgh medical school. Physicians from all over the country contacted him about challenging cases that stumped them. He is said to have INFLUENCED THE WHOLE FIELD OF INTERNAL MEDICINE AND EVENTUALLY HELPED BRING IT INTO THE COMPUTER AGE.
The 1970 “blackjack,” as he was referred to, became "Jack-in-the-Box" as he stepped down as chair of medicine and university professor and devoted himself to developing a computerized method of medical diagnosis. He teamed up with the PITT business medical informatics for a 20-year collaboration! The result of this collaboration was INTERNIST 1, the first computerized diagnostic database. INTERNIST 1 later gave way to QUICK MEDICAL REFERENCE, allowing physicians to interact and check their diagnostic decisions.
During Dr. Gene Myers's (AKA–Geno) internship CARDIOLOGY ROTATION, he fell in love with the program and his professors, now "setting his sights” on being a university professor of cardiology for his life's work.
*Halfway through the PITT internship, during a late night on-call work, Myers received a telephone call from his med school “buddy,” Dr. Jon Dranov. That evening, Jon went on to explain to him that he had spontaneously, without his knowledge, made an application for Geno to transfer to Duke University, where he was to be a medical resident, chief resident, and cardiology fellow! He explained that all the paperwork was completed and “he just needed to show up.” This all seemed to be quite crazy, and none of us had ever heard of such, but in the end, it turned out to be absolutely true. At the completion of Myers's PITT internship, he went on to Durham, North Carolina, and Duke University! 55 years later, he is reported to have asked Jon what made him do this outrageous good deed for him—he just turned to Geno and said, “I thought you would be happier here with me!”
Duke University Medical Center
RESIDENCY (internal medicine) + CHIEF RESIDENT + FELLOWSHIP
(Cardiology) [1970–1973]
Founded in 1925, Duke is ranked 5th in internal medicine, with more than 7500 applicants for 115 first-year medical students.
Upon arriving at Duke, Myers confirmed that the prearranged "Dranov program" was factual. The house staff (interns, residents, and specialty fellows) provided a comprehensive curriculum focusing on developing strong clinicians, effective teachers, and compassionate caregivers with defined pathways for research.
Durham, NC, situated in a rural setting, was an ideal atmosphere from the learning perspective: outstanding professors, intelligent, driven classmates, and strong infrastructure in a large population of patients needing quality healthcare. While at Duke University, Myers recalls 3 unique, memorable experiences.
Bruce W. Dixon, MD (1939–2013) Experience

")
Bruce was a unique individual in many aspects of life. He was a lifelong bachelor, with no siblings—his medical work was his life. His trademark hush puppy shoes, narrow black tie, French cuffs, crew-cut blonde hair, and wire-rimmed glasses told the whole story. He was a Duke chief resident in 1970, 2 years before Myers, and was director of house staff during Myers's era. He was a nationally recognized clinical diagnostic expert but was totally unpretentious. Bruce taught Myers and his colleagues a simple principle of self-continued medical education: Each day, "select a patient from rounds and spend an hour or so each night studying all characteristics of the case". "That way it will always be in your databank of memory". Myers relates a Dixon-case memory of a tobacco farm worker who came into Duke Hospital in a coma, for no apparent reason. Vital signs were nearly normal, but family members stated that he had had abdominal pain, cramps, and spasms before going into a coma. Dixon took Myers to reexamine the patient each day, and on the third evening rounds, the patient awakened, still with no diagnosis. Dixon was emphasizing the "necessity for repeat physical exams, and historical assessments, and to always ask the patient what they believe to be the cause for the malady". The patient, now awake, sat up and boldly stated, "I can tell you exactly what happened and what the problem is". "I sat on my outhouse seat, and she bit me twice"; Who bit you? Myers asked. -- Answered the patient—the black widow spider who lives there.
Then Dixon asked the patient if he could show us the spider and help us to capture it so that it could be used in the weekly Grand Rounds 2 days later. Without hesitation, the gentleman agreed. That Grand Rounds featured the live specimen in a controlled environment and a lecture by North Carolina-based Raymond W. Thorpe, who wrote a definitive book—BLACK WIDOW: AMERICA'S MOST POISONOUS SPIDER.
Walter Kempner, MD (1903-1997); Duke Rice Diet and the Dr. Jay S. Skyer Experience


Walter R. Kempner, a brilliant young scientist, was brought as a refugee from Nazi Germany to join the faculty of Duke Hospital's Department of Medicine in 1934. Following his first AMA rice diet presentation in 1944 on the origins and treatment of metabolic diseases, diabetes mellitus, and kidney and heart failure, patients flocked to Durham, North Carolina, for treatment. The headline-grabbing success of Kempner's rice diet contributed significantly over the years to Durham's economic growth and transformation into a world-famous center for medical research and care.
He believed that the kidney had two functions: one excretory and the other metabolic, and theorized that if the protein and electrolyte load on the kidney was reduced to a minimum, the kidney might better perform this more essential metabolic goal. At that time, there was no significant treatment for these maladies. The rice diet satisfied the requirement to reduce metabolic demand, resulting in reversal of diabetic retinopathy, CHF, and renal failure.
Myers was introduced to the Kempner programs and their incredible results by a fellow resident, Dr. Jay S. Skyler, MD. To emphasize these remarkable results, he had Myers review the published data and retinal photographs. Years later, Myers used this data to reverse nephrotic syndrome in an obese individual with chronic renal failure using laparoscopic gastric bypass (reducing the load of protein and electrolytes on the kidney), as opposed to the rice diet. To the surprise of all doubters, the nephrotic syndrome completely disappeared.
Skyler graduated in the second Penn State-Jefferson Med School accelerated program, permitting a select few students to complete BS-MD in 5 years versus 8 years.
Dr. Jay S. Skyler, MD, MACP, FRCP went on to become a highly respected Professor of medicine, pediatrics, and psychology in the division of endocrinology, diabetes and metabolism at the University of Miami. He also serves as a deputy director for clinical research and academic programs and diabetes research Institute at the same institution.
Dr. Skyler has had a remarkable academic career spanning more than 5 decades of research and patient care at the University of Miami.
He is best known internationally for advancing the understanding and treatment of type 1 diabetes, especially efforts to prevent or modify the disease before it fully develops.
- Leading the NIH sponsored diabetes prevention trial–type I (DPT–1) for over 20 years aimed preventing or slowing type 1 diabetes.
- Investigating immune modulating therapies to protect or preserve insulin–producing beta cells foundational work toward disease–modifying treatments was one of his specialties
- Promote meticulous glycemic control and patient self-management including insulin dosing "algorithms" that helped shape intensive insulin therapy.
- Contributing to clinical trials that led to the first FDA–approved disease modifying therapy for type 1 diabetes
He has been prior president of the American diabetes Association (ADA) and has authored or coauthored 100s of scientific articles in the book chapters.
ENDURING INFLUENCE: Overall, Dr. Skyler’s Legacy includes transformative contributions to diabetes research, clinical care, education and national scientific leadership–particularly in type 1 diabetes prevention and care. Many practitioners and researchers around the world continue to build on his work.
James T. Chen, MD (Cardiac Radiologist) Experience: (1924–2006)
 Myers recalled that Dr. Chen was a professor of radiology at Duke University Medical Center, specializing in cardiothoracic radiology, and taught Myers the technique and details of cardiac fluoroscopy. During this time, Myers learned of the major importance of CORONARY CALCIFICATION, detected by simple fluoroscopy—while very few cardiologists recognized its significance. The data collected during the early 1970s was eventually evaluated and published in 1974, revealing the POWER OF SIMPLE FLUOROSCOPY IN ASSESSING CORONARY CALCIFICATION. In detecting coronary artery disease (CAD), among patients in whom coronary calcification was identified, 97% had >70% stenosis. This relatively brief learning experience left an indelible mark on Myers, as he implemented this new knowledge from day one in his private practice in Sarasota, Florida.
Myers recalled that Dr. Chen was a professor of radiology at Duke University Medical Center, specializing in cardiothoracic radiology, and taught Myers the technique and details of cardiac fluoroscopy. During this time, Myers learned of the major importance of CORONARY CALCIFICATION, detected by simple fluoroscopy—while very few cardiologists recognized its significance. The data collected during the early 1970s was eventually evaluated and published in 1974, revealing the POWER OF SIMPLE FLUOROSCOPY IN ASSESSING CORONARY CALCIFICATION. In detecting coronary artery disease (CAD), among patients in whom coronary calcification was identified, 97% had >70% stenosis. This relatively brief learning experience left an indelible mark on Myers, as he implemented this new knowledge from day one in his private practice in Sarasota, Florida.
From Duke University, Myers went on to Georgetown University in Washington, D.C.
Georgetown University Hospital Cardiology Fellowship (Adult Pediatric) [1973-1975]
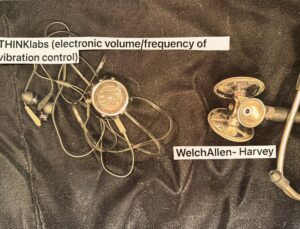
 In 1973, Myers made one more educational relocation in order to pursue a Dr. Proctor Harvey–inspired experience at Georgetown University Medical Center, focusing on clinical skills, patient-centered care, and teaching excellence, as these were the aspects of Dr. Harvey's program. Dr. Harvey created and built a division of cardiology and established a cardiology fellowship program that became a model for programs at other teaching hospitals. Myers recalls that, as a cardiology fellow, he and his peers were responsible for Harvey's weekly teaching conferences, which featured electronically amplified sounds and chest wall movements of actual patients on stage while the audience (usually 300–400 physicians) from surrounding areas could appreciate these physical findings using Harvey's mechanical devices. These conferences became standing-room-only events, attracting physicians from all over the nation and world. Myers recalls the unique introduction to Dr. Harvey's improved stethoscope and innovative audiovisual approaches to teaching cardiology, which were unique to Georgetown at the time. Harvey reinforced his emphasis on direct examination of the patients as opposed to technological procedures and cardiac catheterization. "Harvey's rule": Your ears are better than any test and do not cost the patient a cent" (echo had just been invented and introduced). By the middle of the fellowship, he recalls that all of the fellows had become highly proficient in cardiovascular clinical evaluation, having been exposed to nearly all cardiac disease states.
In 1973, Myers made one more educational relocation in order to pursue a Dr. Proctor Harvey–inspired experience at Georgetown University Medical Center, focusing on clinical skills, patient-centered care, and teaching excellence, as these were the aspects of Dr. Harvey's program. Dr. Harvey created and built a division of cardiology and established a cardiology fellowship program that became a model for programs at other teaching hospitals. Myers recalls that, as a cardiology fellow, he and his peers were responsible for Harvey's weekly teaching conferences, which featured electronically amplified sounds and chest wall movements of actual patients on stage while the audience (usually 300–400 physicians) from surrounding areas could appreciate these physical findings using Harvey's mechanical devices. These conferences became standing-room-only events, attracting physicians from all over the nation and world. Myers recalls the unique introduction to Dr. Harvey's improved stethoscope and innovative audiovisual approaches to teaching cardiology, which were unique to Georgetown at the time. Harvey reinforced his emphasis on direct examination of the patients as opposed to technological procedures and cardiac catheterization. "Harvey's rule": Your ears are better than any test and do not cost the patient a cent" (echo had just been invented and introduced). By the middle of the fellowship, he recalls that all of the fellows had become highly proficient in cardiovascular clinical evaluation, having been exposed to nearly all cardiac disease states.
 To complement the live patient experience, Dr. Harvey had enlisted the assistance of William (Bill) Clifford Roberts, MD, a world-renowned cardiovascular pathologist. He had a most unique background, for even though he was a clinical cardiac pathologist, he had a medical internship and became highly proficient in both. Dr. Bill Roberts was recognized as a truly world-class teacher. To accomplish this, he established a system whereby dozens of institutions around the nation, and in particular Washington, D.C., each month sent him cardiac autopsy specimens, and in return, he completed autopsy results and reports and sent them back to the parent institution. During these years, he was studying up to 50 hearts per month!
To complement the live patient experience, Dr. Harvey had enlisted the assistance of William (Bill) Clifford Roberts, MD, a world-renowned cardiovascular pathologist. He had a most unique background, for even though he was a clinical cardiac pathologist, he had a medical internship and became highly proficient in both. Dr. Bill Roberts was recognized as a truly world-class teacher. To accomplish this, he established a system whereby dozens of institutions around the nation, and in particular Washington, D.C., each month sent him cardiac autopsy specimens, and in return, he completed autopsy results and reports and sent them back to the parent institution. During these years, he was studying up to 50 hearts per month!
- We, the Georgetown fellows, benefited from his mega-effort, as weekly he would bring "buckets of human hearts" to our clinical–pathology fellows’ conference for the fellows’ inspection and study.
 However, Roberts always "turned the table on us," since after studying the pathological specimen, we now had to "guess the history that went with the specimen"! During Myers’ time at Georgetown, he had the opportunity to evaluate congenital heart defects with Dr. Roberts and published an article with him.
However, Roberts always "turned the table on us," since after studying the pathological specimen, we now had to "guess the history that went with the specimen"! During Myers’ time at Georgetown, he had the opportunity to evaluate congenital heart defects with Dr. Roberts and published an article with him.
- Despite these awesome cardiac, physical exam, clinical, and pathology experiences, Myers most vividly recalls the lesson that cast the greatest lifelong influence from the Harvey fellowship: a practice known by Dr. Harvey as the G/T RATIO. This practice, unique to Dr. Harvey, had everything to do with the heart and nothing to do with cardiology! Dr. Harvey’s G/T RATIO, of course, was infinite—all give, no take—and Harvey lived his life by this ratio. His love was selfless and unconditional, and it understood and accepted imperfections. Since his "Harvey days," Myers has done his best to perpetuate this philosophy to all who will listen.
- After 10 years (1965–1975) of uninterrupted glorious medical education, it was time for “payback”: United States Naval military service, under the BERRY plan.

Military Service
[United States Navy] (1975–1977)
 Portsmouth Navy Regional Medical Center (PNRMC), Portsmouth, Virginia
Portsmouth Navy Regional Medical Center (PNRMC), Portsmouth, Virginia- Lieutenant Commander—USN and Assistant Professor of Medicine, Eastern Virginia Medical School (EVMS), and Discovery of a New Disease while in the USN:
- As the Navy's oldest, continuously operating Hospotal since 1830, Naval Medical Center Portsmouth (NMCP) proudly serves past and present military members and thier families. The nationally acclaimed, state of the art Medical Center, including its 10 branch and TRICARE Prime clinics located throughout the Hamptons Roads area, additionally offers premier research and teaching programs designed to prepare new doctors, nurses and hospital corpsman for future roles in healing and wellness. NMCP is a patient-driven Triacre facility entrusted with the health readiness of the United States Armed Forces.
- On historic Hospital Point in Portsmouth, Virginia, the main campus of NMCP is home to more than 5000 men and women who provide healthcare serivces to the brave men and women of our Armed Forces, their familits and military retirees, over 420,000 beneficiaries.
- BERRY Plan: Military service deferment. Myers recalls fortunately being part of the U.S. BERRY Plan (1954–1980), a Vietnam War–era program in the United States that allowed physicians to defer (all physicians) from obligatory military service until they had completed medical and residency training. During that era, all physicians had to serve in the military or Public Health Service, but the BERRY Plan offered options on where they would serve. He was fortunate that the plan let him complete all of his training, including internship, residency, and cardiology fellowship specialty training.
- In 1975, he was assigned to the cardiology section of Portsmouth Navy Regional Medical Center in Portsmouth, Virginia. He recalls having no idea what to expect, even after having been in the ROTC (Reserve Officer Training Corps) at Penn State University. However, he explains that it was a wonderful "eye-opening experience" in all ways, now believing that every U.S. citizen should have to serve in one capacity or another. There, he had the opportunity to grow his adult-pediatric noninvasive and invasive procedural and teaching skills.
- While serving in the United States Navy as a lieutenant commander at PNRMC, he was selected as an assistant professor of medicine at Eastern Virginia Medical School (EVMS), Norfolk, Virginia.
- U.S. Navy Community Service: Buckets of human hearts, brains, and livers to the rescue! The captain and cardiologist in charge of the cardiology section at PNRMC suggested that Myers and his peers offer some sort of community service to the Portsmouth and Norfolk areas. After considering several options, he settled on Narcotics and Alcohol Anonymous 12-step programs. This seemed like a good choice since the problem was quite prevalent in both the civilian and military communities, and the captain agreed.He recalls giving substantial thought as to how he could make a unique and memorable impact on participants. Then it came to him—just as Dr. Bill Roberts, the world-renowned cardiovascular pathologist, made a huge impact on the Georgetown cardiology fellows by bringing buckets of hearts to the weekly clinicopathologic conference, Myers would procure a bucket of human cirrhotic livers, brains, and hearts to present at the 12-step programs.

Both the captain of the cardiology section and the admiral of PNRMC approved. He recalls that after his first presentation at a 12-step program, it was always standing room only thereafter. This activity then occurred monthly, and many attendees reported that this vivid presentation helped them on the road to recovery.
Curiosity prevailed, and he pursued all other possible diseases and eventually created a new differential diagnosis list. A complete physical exam, rather than just a cardiovascular-directed exam, led to discoveries. This group of patients had a similar constellation of symptoms and physical exam findings to those with classical angina pectoris. However, physical exam features also included loss of cervical range of motion, sensory deficits in the anterior chest and arm, reduced handgrip, and, in some cases, cervical rotational precipitation of reproducible symptoms. Shortness of breath was common, but only with arm exercise, not leg exercise. Myers recalls finding four physical exam maneuvers that could usually reproduce the symptoms.
Furthermore, nitroglycerin under the tongue frequently relieved the symptoms, as it does with normal obstructive coronary artery angina pectoris. He concluded that the symptoms were not cardiac at all but related to cervical spinal cord compression, also involving the nerve exits (foramina) to the arms. This unrecognized disease scenario deserved a memorable name so physicians could remember to include this diagnosis in patients with chest-arm pain and shortness of breath.
Naming the disease was straightforward: cervico (neck), precordial (area over the chest wall directly over the heart), and angina (type of chest discomfort usually caused by reduced blood supply to the heart muscle). It is easy to remember because the acronym spells CPA (like Certified Public Accountant).
This data was presented live at a major session of the American College of Cardiology annual meeting and thereafter published in peer-reviewed journals. When asked by one of several hundred audience participants, "How does arm exercise produce chest discomfort, shortness of breath, and the other symptoms?" he spontaneously responded:
"This is called the 'OSCAR-MAYER-WIENER EFFECT'—arm exercise demands > muscle/nerve blood supply > spinal cord blood flow, and 'swells the spinal cord in an already narrowed canal,' similar to how a hot dog swells when you boil it."
This explanation brought the house down in laughter and applause in an otherwise conservative audience. This presentation and the JAMA (Journal of the American Medical Association) article were picked up by Mr. Lawrence Galton, medical news editor for Family Circle Magazine (then the world's largest-selling women's magazine, as advertised in 1977), where he reported "chest pain from a neck ill," creating substantial national and international notoriety.
Chief of Cardiology: University of South Carolina School of Medicine, Columbia, South Carolina
- .In 1977, at age 33, as a lieutenant commander, Myers completed his tour of duty in the USN and was recruited by Dr. Victor Murdock, a nephrologist he had met at PITT during his internship, who was now the chairman of the Department of Medicine at the new medical school in Columbia, S.C. Myers was slated to be the first chief of CARDIOLOGY for the new medical school.
- After 13 consecutive years (without a “gap year”) of educational and intellectual pursuit, and the lifelong goal to be a teaching professor and youngest chief of a cardiology section at a university, he recalls feeling like he had just arrived at his destination. He purchased two properties in Columbia, S.C. Then the reality of this esteemed position set in. The workload was easily handled, but the slow pace of committee decisions and the administrative burden felt overbearing and boring, plus there was very little time for patient contact. Suddenly, he realized he was not “cut out” for such an administrative position, although it had been his lifelong goal—he recalls thinking to himself that he just did not have the administrative "mind-set" and concluded that this was not an “acquired taste”! Despite the fact that this was the 13th move since he graduated from medical school, he knew change was imminent. At that moment, he realized that it was important to choose a geographical location where he wanted to live and spend the rest of his practicing life. In other words, choose a location where you want to live so that, just in case you die prematurely, you will have "lived the dream."
- At 60, Myers began to understand the origins of a dream he had carried since childhood-the ambition to become the youngest academic chief of cardiology in the country. In hindsight, that goal appeared less a personal invention and more an unconscious inheritance. His father had once pursued the same aspiration, and young Myers, perhaps without realizing it had echoed it - a quiet effort to live up to expectations and avoid disappointment.Psychologically, it was later described as a form of family "REPETITION COMPULSION", a pattern in which unresolved ambitions pass silently from 1 generation to the next.Then came Mentors McCloskey & McCloskey. Recognizing the weight young Myers still carried, he intervened not with lectures, but with wisdom-–offering the poem THE GUY IN THE GLASS by Dale Wimbrow (1895-1954). Its message of self–honesty and inner peace, mentor McCloskey believed, would help free Myers from lingering guilt and the invisible pressures of pleasing both father and professors alike. And boy was he right!
 "The Guy in the Glass" delivers a powerful message about SELF-RESPECT, INTEGRITY AND SELF ACCEPTANCE.Wimbrow wrote the poem to express the importance of living a life that is true to oneself rather than seeking approval or validation from others (in other words, "be your self-everyone else is taken). It has since been widely shared and referenced in various contexts, particularly in discussions about personal honesty and self-respect.This poem was propelled to fame after an "18–-year-old boy wrote a letter to the editor of the American Magazine in 1934, 1 good reason, please, "he asked, why an ambitious young man should be honest". The publisher invited readers to answer him. Thousands of replies poured in and one of these was from DALE WIMBROW, who sent in "The Guy in the Glass" poem, to answer the young man's question. The words impressed the editor of the American Magazine so much that they published it-and you know the rest of the story!The rhyme schema of the poem is AABB. An AABB rhyme scheme refers to a set of four lines in which the first two lines ends with words that rhyme with one another, followed by lines three and four which also end with words that rhyme with one another. There have been some versions of the poem made into music, including a James Brown version and a Brooke Bilker version.Michael Jackson's "man in the mirror" (1988) and Peter Dale Wimbrow’s "the Guy in the Glass” poem (1934) both center on the theme of self–examination as the catalyst for personal change. While Jackson's song focuses on using interval change to improve the world, the poem emphasizes staying true to one's conscience to achieve personal satisfaction.
"The Guy in the Glass" delivers a powerful message about SELF-RESPECT, INTEGRITY AND SELF ACCEPTANCE.Wimbrow wrote the poem to express the importance of living a life that is true to oneself rather than seeking approval or validation from others (in other words, "be your self-everyone else is taken). It has since been widely shared and referenced in various contexts, particularly in discussions about personal honesty and self-respect.This poem was propelled to fame after an "18–-year-old boy wrote a letter to the editor of the American Magazine in 1934, 1 good reason, please, "he asked, why an ambitious young man should be honest". The publisher invited readers to answer him. Thousands of replies poured in and one of these was from DALE WIMBROW, who sent in "The Guy in the Glass" poem, to answer the young man's question. The words impressed the editor of the American Magazine so much that they published it-and you know the rest of the story!The rhyme schema of the poem is AABB. An AABB rhyme scheme refers to a set of four lines in which the first two lines ends with words that rhyme with one another, followed by lines three and four which also end with words that rhyme with one another. There have been some versions of the poem made into music, including a James Brown version and a Brooke Bilker version.Michael Jackson's "man in the mirror" (1988) and Peter Dale Wimbrow’s "the Guy in the Glass” poem (1934) both center on the theme of self–examination as the catalyst for personal change. While Jackson's song focuses on using interval change to improve the world, the poem emphasizes staying true to one's conscience to achieve personal satisfaction.
The poem has subsequently been frequently recommended when individuals are searching for "self" when hindered by the past.
- A month later, four internists in Sarasota, Florida, practicing at SMH, had heard of his interest in the area and encouraged him to come and visit for a week or so. One of them, an incredibly qualified internist, Dr. Jack Lieberman, felt that Myers would be a “good fit” for the community; at that time in 1977, there were only one or two board-certified cardiologists in town and no invasive interventional cardiologists. Without ever having met Myers, he invited him to come down to Sarasota and stay at his home for two weeks, "until he was sold on Sarasota as his final practice destination.” The four internists, as a group, promised their support and also agreed to permit Myers to make rounds on weekends on all of their patients to get him started.
Private Practice—Sarasota, Florida
(1977– ) Gene E. Myers Cardiac and Vascular Consultants, PA (GEMCVC)
- OPENING DAY: In 1977, he moved to Sarasota and opened his private practice as a solo practitioner. There was no cardiac cath lab, no interventional procedures, and no heart surgery. Only one echo machine was available, owned by a local board-certified, high-quality cardiologist. In his first office, he "shrunk the waiting room" and added a CARDIAC FLUOROSCOPY unit, just as he had learned from Dr. Jim Chen at Duke. In 1977, he was one of the few cardiologists in the country who recognized the power of detecting coronary calcification, understanding that this was the most effective, least expensive, and most available tool for early detection of coronary artery atherosclerosis. Since Myers was trained in adult and pediatric cardiology, he was asked to help with the community-based volunteer congenital heart disease clinic by the director, Dr. Ed Rushton. He served in that position for seven years.
- FIRST CARDIAC CATH (SMH) [1977]: In 1977, the SMH administration was bold and aimed to build a WORLD-CLASS, COMPETITIVE, SUSTAINABLE HEART PROGRAM. Myers, along with a highly trained invasive cardiologist colleague arriving simultaneously in Sarasota, developed plans for the new cardiac cath lab with the blessing and support of SMH administration, Sarasota internists, and local cardiologists. In late 1977, he performed the first cardiac catheterization at SMH.
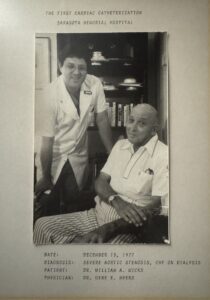
- He recalls that this first patient was a retired physician with severe aortic valve blockage (aortic stenosis, AS) and atherosclerotic coronary artery blockages. In reviewing the benefits and risks with the patient, he frankly explained that this would be the first cardiac cath at SMH, his first case in private practice since the USN, and that it was a high-risk procedure. Myers recalls this physician looking him straight in the face and saying, "Go for it. I have nothing to lose." Fortunately, the case went smoothly. The next day, the patient was transferred to Tampa General Hospital (TGH) for valve replacement and bypass surgery, which was successful. Thoughtfully, the bold SMH administrative team had anticipated transfer needs and built a helipad on the hospital roof.
-
- SMH HEART CENTER HEART SURGERY (1983): The volume of Sarasota County and surrounding county referrals for cardiac catheterization increased rapidly, to the point where TGH kept an operating room available for rapid transfers. By 1983, the Cath Lab volume and referrals for CABG (coronary artery bypass graft surgery) had increased to the point where they exceeded the requirements set by society guidelines to apply for a Certificate of Need (CON) for a heart surgical center.
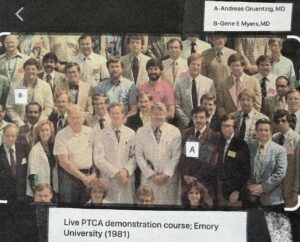
- From SMH First Cath → OJT (On-the-Job Training) for PTCA (Percutaneous Transluminal Coronary Angioplasty): From medical school at the University of Pennsylvania onward, all students were taught the fundamental maxim: "SEE-1 → DO-1 → TEACH-1." In 1977, Myers recalls becoming captivated by published reports of Dr. Andreas Gruentzig (1935–1985) in Zurich performing the first PTCA in the world—hardly able to imagine opening a blocked coronary artery in an awake patient using a balloon catheter. A few months later, on March 1, 1978, Dr. Simon H. Stertzer, MD, at Lenox Hill Hospital, New York City, performed the first PTCA in the USA. Myers carefully monitored the literature until Dr. Gruentzig relocated to Emory University, Atlanta, Georgia, in 1980. By February 1981, Myers began his OJT under the "MASTER INNOVATOR GRUENTZIG," attending his inaugural annual teaching course at Emory. These courses featured live teaching cases each afternoon over three and a half days, significantly advancing the procedure to all 200 worldwide attendees. Soon thereafter, Myers began referring patients from Sarasota to Dr. Gruentzig at Emory University for PTCA.
- "TABLES TURNED": Gruentzig, the "father of coronary angioplasty" and master teacher, faced administrative challenges at Emory and turned to GEMCVC's administrative group for guidance (1982–1983). Dr. Gruentzig and his administrative staff quickly noticed Myers’ organizational techniques, written communication systems, and in-depth patient-specific education letters and cineangiograms (35 mm heart cath movies) for patients traveling to Emory University for PTCA. They also recognized the GEMCVC's consistently high esprit de corps among employees. Gruentzig’s administrator requested an on-site visit to observe the organization’s activities and systems. They observed staff implementation of patient service, patient education, and the personal relationship between physicians, administrators, and the clinical team. They also recognized the value of GEMCVC's no-charge, in-office nursery (since 1978) for employee newborns, which aided in retention of experienced staff. At the conclusion of the hands-on visit, they acknowledged differences between European and American methods from both administrative and clinical perspectives and made positive changes thereafter. [Some systems were inspired by "THE NEW GOLD STANDARD" and the CREDO card: The Ritz-Carlton Company, Joseph A. Michelli.]
 Dr. James (Jim) Robineau Margolis, MD Experience: One of the recognized world pioneers of Percutaneous Coronary Intervention (PCI). At one of the earlier Gruentzig Emory University courses, Myers met Dr. Jim Margolis (1943–2023). Dr. Margolis had previously trained in Zurich and participated in Gruentzig’s 1978 European demonstration courses. By the time Stertzer performed the first American PTCA in 1978, Margolis was not far behind and is credited as the sixth person in the world—and the first in the Southeastern United States—to perform PTCA. He is considered a global pioneer of angioplasty. Jim became a personal mentor to Myers and, by Proctor Harvey criteria, always maintained a G/T ratio substantially >1. He accepted Myers into his cath lab every other Friday for over six months until Myers performed his first PTCA at SMH, with Margolis at his side (he never accepted a stipend, not even for gas).
Dr. James (Jim) Robineau Margolis, MD Experience: One of the recognized world pioneers of Percutaneous Coronary Intervention (PCI). At one of the earlier Gruentzig Emory University courses, Myers met Dr. Jim Margolis (1943–2023). Dr. Margolis had previously trained in Zurich and participated in Gruentzig’s 1978 European demonstration courses. By the time Stertzer performed the first American PTCA in 1978, Margolis was not far behind and is credited as the sixth person in the world—and the first in the Southeastern United States—to perform PTCA. He is considered a global pioneer of angioplasty. Jim became a personal mentor to Myers and, by Proctor Harvey criteria, always maintained a G/T ratio substantially >1. He accepted Myers into his cath lab every other Friday for over six months until Myers performed his first PTCA at SMH, with Margolis at his side (he never accepted a stipend, not even for gas).
Key Certifications
- Internal Medicine (ABIM—American Board of Internal Medicine)
- Cardiovascular Diseases (ABIM)
- Cardiovascular Computed Tomography (CT)
- Certification Board of Nuclear Cardiology