Business Principles and Practices Applied to Cardiovascular Medicine
Myers Style
Early Life
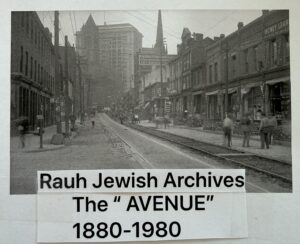 Myers recalls, as a teenager, frequent trips from Penn State to Pittsburgh, "allegedly" to visit his maternal and paternal grandparents. Most occasions included a Pirates baseball game. The real purpose, retrospectively (50 years later), for the frequent sojourns was to visit "FIFTH AVENUE." For nearly a century, Jewish and Arabic commercial activity in Western Pennsylvania centered on a long 9-block stretch of lower Fifth Avenue in the uptown section of Pittsburgh. "The Avenue," (1880-1980) as it was called, was the prime location for the Jewish and Middle Eastern-owned wholesalers that supplied stores throughout the region. The wholesale businesses were strictly commercial enterprises, but their work created long-lasting communal bonds. Young Myers recalls his professor, labor relations negotiator Dad, speaking in Arabic or broken Hebrew, always emphasizing the European technique of establishing friendship and bond before business. He recalls always feeling embarrassed at the end of the communications because 90% of the time Dad never purchased anything—the object was teaching young Myers about the art/science of negotiation! Later in life, he replicated this art by doing the same for his sons and daughter.
Myers recalls, as a teenager, frequent trips from Penn State to Pittsburgh, "allegedly" to visit his maternal and paternal grandparents. Most occasions included a Pirates baseball game. The real purpose, retrospectively (50 years later), for the frequent sojourns was to visit "FIFTH AVENUE." For nearly a century, Jewish and Arabic commercial activity in Western Pennsylvania centered on a long 9-block stretch of lower Fifth Avenue in the uptown section of Pittsburgh. "The Avenue," (1880-1980) as it was called, was the prime location for the Jewish and Middle Eastern-owned wholesalers that supplied stores throughout the region. The wholesale businesses were strictly commercial enterprises, but their work created long-lasting communal bonds. Young Myers recalls his professor, labor relations negotiator Dad, speaking in Arabic or broken Hebrew, always emphasizing the European technique of establishing friendship and bond before business. He recalls always feeling embarrassed at the end of the communications because 90% of the time Dad never purchased anything—the object was teaching young Myers about the art/science of negotiation! Later in life, he replicated this art by doing the same for his sons and daughter.
The Power and Influence of Mentors
Myers remembers being coached by his dad as a teenager that opinions are a formal expression of judgment and advice by an expert who has studied all aspects of the question at hand and has come to certain conclusions. On the other hand, ideas and thoughts carry much less weight. He concluded that it is best to perfect the art of knowing what one is sure of and also knowing what one does not know. He learned at a very young age that if you tell your mentor "I KNOW," the educational communication dies on the spot. As a young adult, he applied this "rule"—always seek help from others more knowledgeable than yourself. For him, all this boiled down to seeking mentors to guide him through all aspects of life and business. Several influential examples are explored.
 One mentor combo was a lovely couple of Italian heritage, each with a high school education and migrating to the United States as teenagers. Although their level of formal education was "only" high school, they possessed the ultimate in "street smarts" concerning real estate, business, construction, and "wraparound banking mortgages." He met this couple while riding bicycles with them, one year after coming to Sarasota. Together, they formed a business partnership, where this mentor combo had power of attorney for Myers for nearly 20 years while he learned the rules of the street. While his parents thought that he was "nuts," they eventually came to realize it was a glorious love/friendship with a G/T ratio greater than 1 until the day they passed on.
One mentor combo was a lovely couple of Italian heritage, each with a high school education and migrating to the United States as teenagers. Although their level of formal education was "only" high school, they possessed the ultimate in "street smarts" concerning real estate, business, construction, and "wraparound banking mortgages." He met this couple while riding bicycles with them, one year after coming to Sarasota. Together, they formed a business partnership, where this mentor combo had power of attorney for Myers for nearly 20 years while he learned the rules of the street. While his parents thought that he was "nuts," they eventually came to realize it was a glorious love/friendship with a G/T ratio greater than 1 until the day they passed on.
Shortly after meeting mentor Lino, he reviewed Myers real estate holdings that had been purchased prior to their relationship, which consisted of 5 single-family rental homes 4 blocks from Sarasota Memorial Hospital (SMH). He bluntly stated that they were far too distant from the hospital and stated by the time they appreciated we would both be on Medicare! So, he put 3 of the houses up for sale and informed me that the other 2 houses were to be used as rent-free and maintenance free homes for recently arriving legal Vietnamese refugee families, all coordinated through Linos local Catholic Church. This was a 2-year "community service", as he explained. And so it was, and all 3 families as expected became productive citizens of the USA.
In 1980, Myers purchased, under the advice of his mentor, property at 2121 S. Tamiami Trail, Sarasota, FL, with the intention of building his first free-standing outpatient office facility. Most of his colleagues thought that he was crazy, since the prime interest rate reached a record high of 21% in December 1980. Nationally construction came to a screeching halt, construction materials were accumulating with no one to purchase, and craftsmen could find no work. Initially Myers was scared but decided that the mentor knew best. Realizing that the real estate/business neophyte appeared perplexed, the mentor boldly explained that this was an ideal window of an opportunity from a construction perspective. Retrospectively, Myers recalls that there was no China or other major international competitors’ competiting for USA produced materials at that time. Furthermore, he explained, this very high prime interest rate would likely last no more than 24 months, at which time we would just refinance at the lower rate. When a close friend/patient heard of these plans, he insisted he except unsecured financing at 14%, and that is what happened.
Less than 12 months later the building was complete, the interest rate started to fall and by1982 dropped to 12% and the property was refinanced. Mentor Lino was right.
Eight Years later the close friend and patient who provided the building loan, was notified by the IRS that a "movie production tax shelter" that he had bought some years previously was determined to be abusive based on the Landmark Tax Reform Act of 1986 and he needed to pay $2 million within a short period of time to avoid penalties. Myers was advised to reciprocate and provide him with a $2 million dollar loan and was paid back 18 months later.
Some years later on Myers behalf, Lino had put a deposit on property at 2540 S. Tamiami Trail and start the process to build a larger facility, that could accommodate all the menu of outpatient services and outpatient cardiac Cath lab. The properties included a main 9500 square foot building and multiple–out-partials and included the entire block on The South Tamiami Trail between Boyce and Morris streets. This new adventure provided several new mentor–student learning experiences.
Lesson1: "Believe your mentor": An architect was hired to evaluate the existing structures and provide recommendations. His conclusions and recommendations suggested that the 2 existing structures were not of value, and all existing structures should be demolished and "start from scratch". Myers remembers being most dismayed at this complex challenge. Recognizing that this appeared overwhelming to Myers, the mentor unequivocally stated that "this architect is nuts and does not know what he is talking about! "Mentor Lino had an uncanny ability to see architectural elements that others would miss and also had in-depth experience having remodeled such structures. With just this visual inspection he went on to explain that there was 1 main support wall serving both buildings–"we will dig a deep bold footer all the way around the perimeter of both buildings and then construct large masonry columns on the footer and then run heavy support I-beams from front to back" spanning the entire width. Recognizing that medical practices must be nimble and have the ability to change as technology changes, this format would permit changing interior walls and rooms with ease.
Lesson 2: during construction a fire occurred as a licensed plumber using a torch to join 2 wall plumbing pipes lighted the 2 x 4 wood structures on fire. The fire covered moderate area, and it was clear this was going to delay completion of the project and get a Certificate of Occupancy. Again, Myers was dismayed, feeling the pressure, since the other building was already sold! Myers was most upset and suggested that this plumber should be fired on the spot. Lino turned to Myers and said with his broken Italian- English " are you a total knucklehead" -do you really want to fire this hard working person with a family and kids just because of this incident? Besides, don't you know that we have a contstuction inurance policy that will likely cover this?"
 A second mentor couple came into his life shortly thereafter. This powerful couple, again with high school educations, became his major influence regarding life’s personal lessons, living as a couple, business lessons, and managing multiple businesses and construction contemporaneously. Initially, they were both patients before becoming lifelong friends and protectors. That all changed when they spontaneously and unknowingly came into the office one day after work and told us that they had performed a "silent shopper" evaluation for the GEMCVC practice. They reported that the six physicians working in the practice had far too many FTEs (full-time employees), and it was not clear what all of these employees were doing—51 FTEs to be exact.
A second mentor couple came into his life shortly thereafter. This powerful couple, again with high school educations, became his major influence regarding life’s personal lessons, living as a couple, business lessons, and managing multiple businesses and construction contemporaneously. Initially, they were both patients before becoming lifelong friends and protectors. That all changed when they spontaneously and unknowingly came into the office one day after work and told us that they had performed a "silent shopper" evaluation for the GEMCVC practice. They reported that the six physicians working in the practice had far too many FTEs (full-time employees), and it was not clear what all of these employees were doing—51 FTEs to be exact.
They offered two recommendations:
- Discharge (fire) all FTEs, then re-interview and hire only those that were felt necessary, or keep the same status quo and go bankrupt.
- Next, they turned to Myers' wife, Susanne, of a year or so, and asked one important question: "Do you like Prada shoes and bags?" The answer was a resounding YES—they responded, "You better get your butt involved in this business before it goes bankrupt!" As a graduate RN, she had very little business experience. The mentors responded, "No problem, we will take care of that," and for the next 365 days, they spent 1 to 2 hours/day "teaching her the ropes," and the rest was history. She became the Mama Bear, large and in charge of all business operations permanently.
Myers recalls meeting Mr. Paul Shabty for the first time, as a patient in 2010. Shortly thereafter they found that they had many common interests. Shabty was a key consultant involved in providing expertise related to renal dialysis services and the manufacturing of medical devices and equipment for the CCM group.
With the CPC of America, Incorporated, company, he was a co-founder of the CPC organization and coinventor of the CPC/CPCA 2000 external counter pulsation technology (ECP). The device was in the end stages of development, when Paul asked Myers to help design the thigh compression cuffs. He agreed to help and with the assistance of his old friend/mentor Dr. Jim Margolis, MD at Miami heart Institute, to accomplish the task providing engineering drawings for the thigh cuffs, expediting completion of their system device. This sealed a lifelong friendship with Mr. Shabty and the Myers medical organization.
With a strong military experience and expertise in interrogation Shabty worked with the Myers organization interviewing all applicants and vendors to the Gene E Myers cardiovascular consultants company-his judgment was never wrong!
Prior to 2010 CPC of America, inc. , over the counter PUBLICLY TRADED stock, company acquired Myers Med Close TM (method and apparatus for arteriotomy closure) patterns, prototype's, normal studies and technology.



William Lawrence Shirer (1904-1993): LESSONS LEARNED FROM PATIENT CARE

Just after Christmas in 1980, Myers recalls receiving a call from a gentleman’s assistant, whom he believes was Mrs. Mary Thomas. She was calling about a man from Massachusetts who had just arrived in Sarasota for rest and “sun time.” At first, neither the town of Lenox, Massachusetts, nor the patient’s name meant anything to him. Old office records later confirmed that this occurred on a Saturday afternoon, January 5, 1980, when the office would normally have been closed. Because the caller was clearly concerned, Myers agreed to meet them in the office that afternoon.
According to the patient and his assistant, the man had no symptoms, but he was concerned about abnormalities on a recent stress electrocardiogram performed in the North shortly before his trip to Sarasota. Both were quite certain that he had no chest pressure, heaviness, tightness, fullness, burning, or discomfort in the arms, jaw, or back, either at rest or with exercise.
At that moment, Myers recalls pausing long enough to remember the words of his University of Michigan mentor, Professor Edward Dodd Robinson, M.D. (1911-1988)(Chairman Department of internal medicine), who taught him that patients often give the most accurate answers when we ask the simplest questions.
With that in mind, and recognizing that the mind is often protective—subconsciously minimizing or overlooking symptoms that may suggest serious disease—Myers changed his approach. Rather than continue asking standard leading questions, he asked, “What would you say is the most strenuous activity you perform, either daily or periodically?”
The answer came immediately and without hesitation: “Shadowboxing.”
Although the answer was specific, Myers did not yet have a clear picture of what the patient meant, nor whether it truly qualified as meaningful physical exercise.
“Bill,” as Myers came to know him, explained that during the war, while reporting from Germany and other regions, he had often been confined to a very small living space. It was unsafe to go outside because of the hostile environment. As a result, he exercised indoors by shadowboxing while standing, using a dim backlight cast against the wall—something he intentionally kept faint so as not to attract military attention. The backlight created moving shadows of his arms, allowing him to exercise discreetly in a confined space.
This was, in fact, quite strenuous and highly aerobic exercise. Upper-extremity exertion places major demands on cardiac output, as the arms require substantially more oxygen per gram of tissue than the legs.
This insight prompted Myers’s next question:
“How long were you able to do this activity during those years?”
Bill answered, “At least one continuous 30-minute session, several times per day.”
Myers then asked, “How long can you do it now?”
He replied, “Only two or three minutes.”
When asked what limited him, he simply said, “My arms get tired.” He did admit to minimal shortness of breath, but no other symptoms. He also noted that his recovery was relatively quick—approximately three to four minutes.
At that point, it became apparent to Myers that the marked decline in exercise capacity, expressed mainly as early arm fatigue, was likely due to an inability to meet the increased cardiac demands of upper-extremity exertion. This strongly suggested significant obstructive coronary artery disease.
Later that same day, they proceeded with what Myers refers to as “cardiac fluoroscopy,” a concept taught to him by his mentor, Dr. Jim Chen, a cardiovascular radiologist at Duke University. As expected, imaging revealed that all three coronary arteries were heavily calcified, implying a high statistical likelihood (85%) that at least one vessel contained a critical stenosis of similar severity.
A simple stress test then reproduced the abnormal findings previously observed by the physician team in Lenox, Massachusetts.
The following week, cardiac catheterization and coronary angiography revealed:
- All three major coronary arteries had severe obstruction, greater than 85% to 90%.
- The disease was not localized, but diffuse, involving most of the length of the arteries.
This created a far more difficult surgical problem, because successful coronary artery bypass grafting requires a suitable downstream target area in the coronary artery where the bypass graft can be sewn in. Coronary angioplasty and stenting, of course, were not yet mainstream, but would not have been applicable for the same reasons.
This dilemma required a different surgical solution, one available at only a few centers in the world. One of the few cardiac surgeons who could consistently perform successful coronary endarterectomy was Dr. Dudley Johnson at Mount Sinai Medical Center in Milwaukee, Wisconsin.
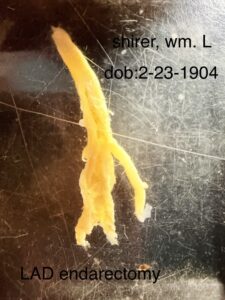
In this procedure, the surgeon opens a long segment of the coronary artery containing diffuse atherosclerotic plaque and then carefully and slowly removes the plaque—and the plaque extending into the branch vessels—in one piece. After that, a segment of leg vein graft is connected to the ascending aorta. The downstream portion of the graft is then split lengthwise and applied over the opened coronary artery as a new roof, a procedure termed vein patch angioplasty.
Dr. Johnson was unusual in that many of his patients undergoing this complex operation had coronary angiography before discharge to confirm that the vein graft reconstruction was successful.
Whereas routine bypass surgery for localized disease might require only three to four hours, this operation lasted eight to ten hours. Because of the prolonged procedure and anesthesia, mental and physical recovery required nearly six months before baseline was regained.
Later, Myers learned from others that Mr. William L. Shirer had chronicled Hitler’s Nazi Germany, had published the monumental work The Rise and Fall of the Third Reich, and had been a preeminent foreign correspondent, along with Edward R. Murrow, helping pioneer broadcast journalism during World War II.
In time, Myers and Shirer also discovered that their birthdays were exactly 40 years and 1 day apart: February 23, 1904, for Shirer, and February 24, 1944, for Myers. Their friendship grew thereafter, and through that friendship Myers, as a scientist and physician, had the opportunity to meet an entirely new community of musicians, writers, and artists in Shirer’s hometown of Lenox, Massachusetts—home of Tanglewood and the Boston Symphony Orchestra.
CONCEPTS REALIZED:
- Patients often give the most accurate answers when physicians ask the simplest questions.
This case taught Myers to avoid leading questions—questions in which the answer is already embedded—because they make it too easy for the patient to respond automatically, without reflection.
- The mind is inherently protective.
Patients may subconsciously minimize, rationalize, or overlook symptoms that could indicate serious disease. The physician must therefore probe gently, thoughtfully, and from different angles.
- A spouse, relative, friend, or surrogate can be invaluable.
This case reinforced the importance of encouraging patients to bring someone with them, since others often notice symptoms, limitations, or changes the patient may not fully recognize or report.
- Patients often come to the physician hoping for reassurance, while the physician’s duty is deeper.
Many patients want to hear that “everything is okay.” Our responsibility, however, is to explore the history carefully, qualitatively, and compassionately in order to identify the true underlying cause—the root driver—of the patient’s problem.
Here is a slightly more memorable version of the section, concepts realized:
Lessons Learned
1.) the simplest question often yields the most truthful answer.
2.) patients may unconsciously protect themselves by minimizing important symptoms.
3.) A companion (medical surrogate) in the room may reveal what the patient does not.
4.) the physician’s task is not merely to reassure, but to uncover the true cause with gentle persistence.
Depicted below, is the diffuse long atherosclerotic plaque removed from the left anterior descending coronary artery, permitting a new roof to be created by the saphenous vein bypass graft.
Southeast Nuclear Medicine Consultants, Inc. (Semnc) (1983)
Myers recalls that the dawn of noninvasive nuclear cardiology imaging began in the late 1970s to early 1980s. At that time, the great majority of physicians performing these services were radiologists with nuclear licenses. He was a very early adopter and visited Drs. Barry Zaret, Strauss, and Wackers at Yale University to fully comprehend the impact of this technology on a cardiology practice. On the first day there, he saw an old Pitt intern classmate, Dr. Elliott Livestone, a gastroenterologist, who promptly canceled Myers' hotel reservation so that he might stay with them (eventually Livestone moved to Sarasota and practiced gastroenterology until retirement).
Having become convinced of the permanency and importance of the technology, he went on to obtain the training necessary to become certified and licensed in nuclear medicine/nuclear cardiology. By 1979, he had opened one of the first outpatient free-standing nuclear cardiology labs on the Florida West Coast. Physician adaptation was somewhat slow, leaving radiologists to perform and interpret these studies. Myers discussed the idea of distributing the technology throughout Central and South Florida using shared responsibility between physicians and end-users via the SENMC company. This 1979 concept permitted the end-user to schedule the procedure, enter all important clinical data, provide appropriate ICD disease codes and CPT procedure codes, perform the clinical procedure, and then transfer all the data on a single "desktop computer" to SENMC. There, Myers would interpret the study, create the report, and send it back to the physician end-user on the same desktop computer.
Only one problem—such a system did not exist in 1983, so he contracted with a California computer software engineer and wrote the contents for the protocol while the engineer produced the software and device. Within 18 months, starting in 1983, they successfully carried out the plan and opened multiple centers in Central and South Florida. Eventually, a South American organization operating in the area discouraged the existence of the organization.
Heart and Vascular Center at SMH (1983)
The SMH cardiac cath lab facility, with very low complication rates, was widely accepted in Sarasota County and surrounding counties. The volume of cardiac cath lab cases rapidly expanded, and a "well-greased" helicopter transfer portal was established between the SMH Cath Lab and Tampa General Hospital (TGH) operating room, prevailing from 1977 to 1983.
As the Cath Lab volume grew and the need for coronary artery bypass graft surgery (CABG) increased, the administration and community physicians realized that SMH heart surgery would eventually be a necessity. The administration worked closely with a group of cardiologists and internists to form a selection committee to find the best young heart surgical talent in the country. In 1983, Drs. Tom Kelly and Don Snyder performed the first SMH open-heart surgery case in a new SMH Tower cardiac surgical facility. The new Tower facility brought the total SMH beds to 825.

Cardiac Diagnostic Imaging Associates (CDIA) (1985–1989)



First outpatient free-standing cardiac cath lab in an ASC (ambulatory surgical center) in the USA (1985).
Evolution of Ambulatory Surgical Centers (ASCS)
Prior to the 1980s, virtually all surgery was performed in hospitals. Waits of weeks or months for appointments were not uncommon, and patients typically spent several days in the hospital and several weeks out of work recovering. The first ASC facility was opened in Phoenix, Arizona, in 1970 by two physicians who saw the opportunity to establish a high-quality, cost-effective alternative to inpatient hospital care for surgical services. Medicare recognition and reimbursement, however, were lacking.
In 1977, Dr. Jerry Maida, MD, a Florida ophthalmologist, helped pioneer outpatient cataract surgery. By 1985, Maida continued to develop the outpatient surgical center model.
1983
Using the Myers innovative "Steward/Mentor" office model described earlier, the MYERS GROUP opened a free-standing, office-based cardiac cath lab, performing cardiac catheterization, coronary and peripheral angiography, and peripheral angioplasty. Additional concierge services included a newly remodeled home adjacent to the medical facility, where the patient's family and friends could stay overnight without additional expense.
CMS "GETs IT": The importance of and reimbursement for out-of-hospital surgical services.
"CMS" stands for the Centers for Medicare and Medicaid Services, a federal agency within the US Department of Health and Human Services responsible for administering Medicare, Medicaid, and the Children's Health Insurance Program. CMS sets Medicare and Medicaid rates for reimbursement for healthcare providers and institutions such as hospitals. In 1985, the United States allowed Medicare-funded cataract surgery to be performed on an outpatient basis and adopted its reimbursement schedule accordingly.
This ruling ushered in the area of Ambulatory Surgical Centers (ASCs), transforming cataract surgery from an inpatient hospital-based operation to an outpatient procedure performed in hospital outpatient departments (HOPDs) or freestanding ASCs. At the same time, physicians faced frustrations like hospital scheduling delays, limited Cath Lab time, and patient overnight stays requiring next-day physician visits and discharge, leading to the development of the ASC.
Certificate of Need (CON) Laws: Obstacles to Hospital Cath Lab and Heart Surgical Center Development.
These regulations required that those who wished to offer new or expand existing services had to first prove to a regulator that the care was needed.
In 1985, all Florida hospitals needed a CON to build a cardiac cath lab, as CON laws were widespread by that time, designed to control costs and prevent unnecessary duplication of services. By 1982, most states had adopted some form of CON program following a federal model. A Cardiac Care Advisory Committee (CCAC) developed criteria for evaluating the necessity for cardiac cath lab facilities, stating that a hospital could demonstrate need if existing cardiac cath labs were operating at more than 90% of their designed capacity.
ASC Benefits
By operating in ASCs instead of hospitals, physicians gain the opportunity to have more direct control over their cardiac invasive services. Physicians can schedule procedures more conveniently, assemble their own concierge-focused skilled staff, and ensure processes and procedures are best suited to their designed facilities tailored to the outpatient setting. This allows professional autonomy over the quality of care as addressed by CMS.
Revelation: Assembling the Pieces to the Puzzle
Myers recalls actively monitoring CMS regulatory changes with frequent trips to CMS Jacksonville, noting several subtle and little-known facts that turned on a "bright light whose time had come."
- First, the important ophthalmologist push toward outpatient non-hospital cataract surgery resulted in CMS reimbursement for the outpatient surgical coded procedure.
- The new declaration by CMS of the ASC recognition "Point of Service (POS)" to identify Medicare reimbursement at this location was a "total game changer."
- At the same time, all healthcare facilities and providers considered cardiac cath lab procedures as "invasive" and not surgical—except Myers.
- Having appreciated the aforementioned, suddenly a bright light went off, realizing that CPT (Current Procedural Terminology) codes used for billing and coding cardiac Cath Lab procedures encompassed surgical codes, as opposed to just medical non-surgical ones.
- What did this mean for cardiac cath labs? Since cardiac cath procedures utilize surgical procedure codes, Myers’ existing office-based, free-standing Cath Lab should be able to apply for an Ambulatory Surgical Center (ASC) license!
In late 1985, a visit to the First Coast Service Options (FCSO), the Medicare administrative contractor (MAC) for Florida in Jacksonville, clarified his position regarding a cardiac cath lab in an ASC. He recalls that initially they queried exactly what surgical procedure was being performed in the CDIA Cath Lab, since they regarded cardiac cath as an invasive procedure, not surgical. However, when the exact CPT codes were identified by the CMS group—codes typically used for cardiac cath lab services—they concluded that since the CPT codes being used for cardiac cath billing reimbursement are indeed categorized as surgical, Myers could apply and make application for an Ambulatory Surgical Center license.
At the same time, Myers’ CDIA freestanding Cath Lab—with pre-op and post-op monitored holding areas and overnight family and friends’ complementary accommodations—was fully operational.
By that time, the facility had a "fine-tuned," concierge-focused professional staff trained in the Ritz Carlton "Golden Rule Methods Book," providing services to non-Medicare and private-pay patients with substantial international referrals. Soon thereafter, Myers recalls undergoing a full CMS inspection and review of the entire office and office-based Cath Lab facility, with an ASC license granted thereafter.
By 1989
SMH hospital's Cath Lab and heart surgical center growth had exceeded all expectations, but SMH had to deal with Florida CON laws and regulations. By then, CDIA was well-established, meeting or exceeding all Medicare, ASC requirements, and CDIA expectations. It was recognized as the first outpatient freestanding cardiac cath lab located in a certified ASC, accredited by JCAHO (Joint Commission on Accreditation of Healthcare Organizations, a US-based nonprofit tax-exempt 501(c) organization accrediting more than 22,000 US healthcare organizations and programs) and AAAHC (Accreditation Association for Ambulatory Health Care, providing accreditation for ambulatory healthcare organizations), ensuring safe and high-quality services to patients. AAAHC had been granted "deemed status" to certify Ambulatory Surgical Centers for Medicare by CMS. Medicare and PRO (Peer Review Organization), established in the 1980s, ensured that services rendered through Medicare were necessary, appropriate, and of high quality.
At the same time, the SMH Cath Lab and Heart Surgical Center were nationally ranked, flourishing with excellent success and high-quality results. With the need for additional cath lab facilities, the hospital faced Florida CON laws and regulations. Eventually, they recognized they could achieve their goal by adding an additional cath lab if they purchased an existing cath lab in an accredited ASC. They proposed an arrangement with CDIA, which was accomplished shortly thereafter. CDIA was purchased by SMH, and with this newly acquired system, the hospital was able to accelerate its growth plans.
Early Adopters of Coronary Artery Laser Angioplasty (1991)
Dr. Myers at SMH and Dr. Alberto Fauci from Saint Francis Hospital in Evanston, Illinois, were the first USA-based interventionalists selected by GV Medical Incorporated to evaluate this device. After performing several cases in Evanston, Illinois, Dr. Fauci came to Sarasota and assisted Myers on the first few cases. The results of their efforts were reported in peer-reviewed journals.
First Report of H2 Blocker Use: This class of drugs, called histamine H2 receptor antagonists (H2 blockers), was used for the prevention of serious Cath Lab radiographic contrast reactions. In 1981, Myers recalls a patient with a history of iodine contrast reaction who, despite prospectively using all recommended prevention measures, including high-dose oral and IV corticosteroids and intravenous antihistamines, developed an intense reaction to Renografin 76 (contrast dye). This reaction did not respond to known measures available at that time. Not knowing what to do next, Myers "broke cardiac cath lab scrub" and called Dr. Frederick Bloom, a highly regarded local immunologist and allergy consultant. His recommendation was to try intravenous H2 blocker, cimetidine (Tagamet), based on a few case reports of its use for other non-contrast reactions. Cimetidine, 300 mg in 100 mL of D5W over 15 minutes, was infused and rapidly reversed the cutaneous and respiratory allergic reaction. Soon after, the Myers-Bloom discovery became a standard worldwide addition to pre-treatment protocols for contrast agent reactions.
First Recognition of Latex Balloon on Swan-Ganz Catheter (1995)
Myers recalls a patient undergoing right heart cath with a Swan-Ganz catheter during postoperative CABG. No iodinated contrast had been administered within 7 days. Two to three minutes after placement in the pulmonary artery, the patient developed anaphylaxis immediately associated with ventricular fibrillation. Initially, it was thought to be secondary to contrast dye, which had not been administered. Further investigation revealed that the Swan-Ganz catheter balloon was made of latex. This represented a re-exposure to latex. In patients with a history of latex allergy, latex-free Swan-Ganz catheters are available by special order. This illustrates the importance of performing a Swan-Ganz right heart cath before contrast exposure to avoid confusing the etiology of anaphylactic reactions.
“Out of Plane” Internal Thoracic Artery (ITA)
Myers noted that in older individuals undergoing catheterization, as the thoracic aorta elongates with age, it tends to buckle. This causes the ITA to arise "out of plane" with the aorta. A catheter was designed with the distal portion out of plane to enable selective catheterization of the vessel. (Patent #)
This device was designed for single-operator use, functioning by debriding the area just above an arteriotomy puncture site, creating a more adhesive surface. A patient-specific autologous fibrinogen was deposited to seal the arteriotomy. The patent and device were acquired by a startup company, followed by an IPO.
Myers developed software for cardiologists to perform billing, coding, report generation, posting, and faxing at the point of service (POS) without human intervention. In 1999, after performing thousands of invasive interventional procedures, Myers concluded that existing systems created a burden. Previously, documentation involved handwritten notes, manual faxing, and multiple staff interventions, often causing delays and errors. Myers collaborated with developers Barry Stutler, Joey Brillantes, Michael Bradford, and Brad Westover to create a tablet-based, standalone software module. This allowed cardiologists to create error-free billing, coding, and reports at the point of service, reducing FTEs from 4.7 to 2.8. The results were presented at American College of Cardiology meetings.
Medicare RAC Audit (Recovery Audit Contractor)
The RAC program, created through the Medicare Modernization Act of 2003, identifies and recovers improper Medicare payments. RAC auditors are paid a percentage of overpayments recovered. Initial audits claimed an 85% error rate for Myers’ physician group. After 10–12 months, the auditors recovered 0% because the automated software module ensured no errors or overpayments.
Cath Lab Software Module vs. Industry Standard (2003)
Medical records from 38 patients who had undergone cath procedures in the previous 12 months were reviewed. Data was scrubbed for privacy and entered into the software module. CPT codes generated were compared to hospital records obtained from dictated reports. Results showed substantial missed CPT codes using experienced hospital staff, causing a financial loss of 29%—demonstrating how hospitals "shorted themselves" due to missed coding.
Prevention Heart Labs Inc
- (PHL): Lessons Learned Regarding STATINS
- By prospectively teaching and counseling patients about ATHEROSCLEROSIS, the "A word," STATIN agents, and the powerful lifetime effects of statins and the PLACEBO–NONCIBO effects, the successful administration of these medications will likely be very high. Simply stated, "education is where it’s at," and the dilemma is how to find the appropriate time and reimbursement to do what is necessary!
- GENETICS Education in PHL
- Educational information regarding laboratory studies to detect familial hypercholesterolemia (FH) & LPA disease and different subgroups of lipids is a necessity. If presented in a thoughtful, easy-to-understand manner, it will be assimilated by most patients.
- LPA Disease: This is a form of "bad cholesterol" made up of two LDL-like particles "hooked together by a sulfur bond." Elevated lipoprotein(a) [Lp(a)] levels are quite common in the general population, with estimates ranging from 20% to 30% of people worldwide. Lp(a) is a unique form of LDL cholesterol and is a strong independent risk factor for cardiovascular disease.
- This GENETIC DISORDER is caused by a "dominant gene." If you have an elevated LPA, each of your siblings and children has a 50% chance of having inherited LPA (based on your genetics only). You have an elevated LPA because one of your parents had an elevated LPA and passed it on to you. The Lp(a) molecule may have "repeat units" called KRINGLE units, and individuals with fewer repeats have up to five times higher levels of LPA (in other words, the number of repeat Kringle units is INVERSELY correlated with LPA levels). Patients of African-American descent have a 2–3-fold greater chance of having this.
- The adverse effects of this disorder are as follows:
(A) Excessive blood clotting (THROMBOGENESIS)
(B) Increased and more AGGRESSIVE ATHEROSCLEROSIS
(C) Increased risk of chronic KIDNEY disease
(D) Increased rate of progression of AORTIC STENOSIS (AS—narrowed, calcified aortic valve)
(E) Associated with INFLAMMATION: While LPA is not a direct inflammatory biomarker, elevated levels are associated with a tendency toward inflammation, particularly in individuals with atherosclerosis
(F) To have this tested, your physician will need to
(G) Request this as a SEPARATE BLOOD TEST because it is NOT included in most standard lipid panels ordered by personal physicians
(H) Diet and exercise have almost no effect on lowering Lp(a) levels
(I) One can have a completely normal cholesterol/lipid panel with a very high Lp(a); i.e., Lp(a) is not part of the standard lipid panel
(J) There is no effective FDA-approved treatment (except a form of "kidney dialysis" called lipoprotein apheresis) for LPA disease, although it has been intensely researched over the past 10–15 years, and a breakthrough is likely in the next few years - HYPERCOAGULATION (Increased Blood Clotting): Myers recalls, around 1998, addressing this predicament. At that time, it was accepted by most cardiologists that atherosclerotic PLAQUE RUPTURE OR EROSION was a significant concern.
We teach that when atherosclerotic plaque develops, it DOES NOT DEVELOP WITHIN THE LUMEN THROUGH WHICH THE BLOOD FLOWS. Instead, it DEVELOPS WITHIN THE WALL OF THE ARTERY. As the plaque grows, it expands toward the outer wall so as not to intrude upon the lumen—this is called remodeling. NEW PLAQUE tends to be SOFT, without a hard surface or scab, and has a propensity to RUPTURE. Statin agents stabilize the plaque and reduce the chance of plaque rupture or erosion. If a plaque rupture or erosion occurs, the contents of this soft plaque become exposed to the bloodstream, and the blood vessel "thinks it has been stabbed from the outside" and forms a clot to seal it off.
Understanding this makes it clear why a patient could have a negative treadmill stress test and still experience a plaque rupture followed by total occlusion an hour later, resulting in a heart attack and sudden death. Excessive clotting is therefore a "big deal." Additionally, clot formed by plaque rupture or erosion may be partially absorbed and incorporated into the plaque itself.
In 1997, there was no organized educational source for cardiologists to learn about clinical hypercoagulation, which tests to order, or how to treat it. Myers began studying hypercoagulation through the book The Medical Clinics of North America: Bleeding and Clotting Disorders for the Internist by Dr. Roger L. Bick, MD. This book was easy to read, even for non-hematologists/cardiologists, and provided practical understanding for everyday application. Dr. Bick, a world-renowned expert, authored over 300 peer-reviewed journal articles and more than 20 medical textbooks. He was also Chief Editor of the Journal of Clinical and Applied Thrombosis/Hemostasis.
Dr. Bick had recently established a private clotting laboratory, was approachable, and served as an outstanding mentor. Over six months, Myers encouraged Dr. Bick to help establish an APPROPRIATE GROUP OF GENETIC/ENVIRONMENTAL (nongenetic) HYPERCOAGULATION TESTS that could be ordered together when hypercoagulation was suspected in precipitating clotting events. Most patients with atherosclerosis, where plaque rupture or erosion and thrombosis was possible, underwent these studies.
After testing, teleconferences with Dr. Bick helped Myers fully understand results and their application to each patient. Although they spoke several times per month, they never met in person until 2006, when Dr. Bick visited Myers in Sarasota after recovering from health issues.
The influence of this world expert profoundly shaped Myers’ approach to patients with atherosclerosis and other cardiovascular diseases. This experience led Myers to develop a specific list of 17 hypercoagulation studies, locally named the BMP–BICK–Myers protocol. Patients undergoing elective procedures where hypercoagulation could impact therapeutics underwent this protocol prospectively.
Deciding which patients should undergo the BMP became simple: one asks, "If this patient had a hypercoagulation state, would it change the diagnostic and therapeutic approach?" If yes, the protocol is recommended. (Estimated Medicare expense for BMP in 2023: $960)
PHL: Lessons Learned and Implementation into Everyday Cardiology Practice
The data and educational results of the Prevention Heart Labs were highly influential, permitting the creation of a heart template for cardiovascular care. Strong educational data emphasizing "the A word" was provided to all patients before initiating therapy for atherosclerosis. Historical data regarding hypercoagulation were obtained, and appropriate laboratory studies were recommended.
HEART-TO-HEART Live Television Show (Blab TV, Channel 40; Sarasota, Florida): In the late 1990s, Myers and Associates aired a LIVE CALL-IN TALK SHOW on Blab TV, Channel 40. The concept of live TV began in Pensacola, Florida, in 1984 and later expanded to Sarasota. The show had a large, consistent viewing audience. The anchor sponsor was a Pittsburgh-based grocery chain contributing $80,000 per year for production. Myers and his partner, Dr. William F. Crick, MD, volunteered weekly without reimbursement as a public service.
MEDICAL INFORMATICS: Myers’ contributions to medical informatics particularly enhanced the efficiency and effectiveness of electronic health record systems.
Dr. Myers is credited as an inventor on several PATENTS related to electronic medical records (EMR) systems. His work has improved accessibility and management of patient health records. ("US Health News"). These patents highlight Myers’ contributions to medical informatics, especially in optimizing the efficiency and effectiveness of electronic health record systems. (“Chat GPT and anonymous”). The hospital "shorted themselves" with missed CPT codes.
AUTOMEDICWORKS, LLC (2000–2009):
In 1999, while on a European business trip, Myers recalls having been captivated by unique service at an outdoor restaurant. First, an attractive waitress took a 3-person order on a handheld device, and there were no errors. Following the meal, the same young lady presented a summary of the services with charges and an area for added gratuity. Finally, a guest signature, with a credit card, completed the transaction with the receipt. There were no intermediaries, no delay, and no errors. On arriving back at Miami International Airport, the identical scenario occurred again at the rental car agency. Eureka, Myers recalls saying to himself; cardiologists need something like this to relieve them of their 5.7 FTEs per cardiologist!. The traditional cardiology practice in 1999, where the cardiologist performed the medical services and dictated the reports and everything else was performed by staff, resulted in medical and coding errors and an unacceptable financial burden. This old-fashioned system in 1999 involved the following: collecting and reading the cardiologist's transcribed report when available and guessing what disease ICD code best describes the data found in the report. This code will be necessary for billing. Next, CPT testing codes must be selected from data in the medical record. Next, the report must be placed in the patient's chart, and a copy sent to referring physicians. Finally, the staff must complete the standard billing form, HCFA (1500) or equivalent. He concluded that all the steps were extremely costly, required increased medical staff, and were subject to errors each time the data was exposed to more medical staff.
The challenges in this old-fashioned system are as follows:
(A) The existing ICD codes were first proposed by Florence Nightingale and then published in 1893 by Bertillon for classification of causes of death—i.e., pathology codes nearly worthless to doctors.
(B) Eventually ICD codes were added for signs, symptoms, and external causes of injury.
(C) So, if it was necessary for the cardiologist to select the proper code, the "book would have to be reorganized", and carried around by the doctor.
(D) Most cardiologists are not interested in typing.
(E) Lack of computer savvy
(F) Apparent unwillingness to change systems
The proposed new automated system eliminates medical staff FTEs and instead provides a system such that the cardiologist, at the point in time of service, can execute the aforementioned.
(A) Have the cardiologist generate the medical report.
(B). Create a system for the addition of the CPT code and ICD code at the point in time of service.
(C) Have the added data "contemporaneously" create billing, coding, report generation, posting the HICFA 1500 charge form, faxing the report,and uploading it into the patient's medical record.
(D) PARAMOUNT OBJECTIVE: Reduce FTEs/Dr., ELIMINATE ERRORS, and POST CHARGES immediately (before going onto the next patient)—all to be performed at the point of time and service [POTS]
RESULTS:
(1) Fortunately, Mr. Barry Stutler, computer/electrical engineer, was there to create the "dream system". He rapidly assimilated a team including Mr. Joey Brillanties, Mr. Michael Bradford, Mr. Brad Westover, and a support team.
(2) $4 million (private equity), and 3.5 years later the task was completed.
(3) Using this cardiology-specific, internet-based, "out of the box system"—conventional or touch screen computers—Automedicworks (TM, Cardioscribe system) was interfaced to a common PMS (practice management system).
(4) Results showed that in just a few minutes or so, the cardiologist at POTS could complete the data necessary to create and submit the final HICFA 1500 billing forms and execute the remaining features discussed.
(5) FTEs to support the cardiologist activity dropped from 4.7-2.8 ---------à the initial objective was satisfied.
(6) PROBLEMS WITH MARKETING:
(A) Conceptually, cardiologists could just not imagine taking the time to perform these "menial tasks" that the staff would have normally performed (2009)—AFTER ALL, THEY ARE DOCTORS, NOT SCRIBES, CLERICAL STAFF, OR CASHIERS!
(B)In 2010 there were dramatic reductions in Medicare reimbursement, and combined, this added up to the reduction in reimbursement of 31-50%!
(C) Realizing , at that time, cardiologist overhead ranged from 60% to 70%, and these reductions resulted in large numbers of cardiology practice BANKRUPTCIES or no profit bailout from hospitals.
(D) Only a few, early adopter practices, withstood the storm unscathed.
(E) Automedicworks, LLC was eventually acquired by a New York firm.